I addressed the question of death lags yesterday in When Will the Exploding Number of Cases Lead to More Deaths?
My analysis shows that states have vastly different lag times. Many people averaged these lags to suggest we are out of the woods.
On top of that mistake, others believe that more testing is behind most of the rise. That has been widely disproved but people will believe what they want.
It’s Not Just Testing
For discussion, please see It’s Not Just Testing
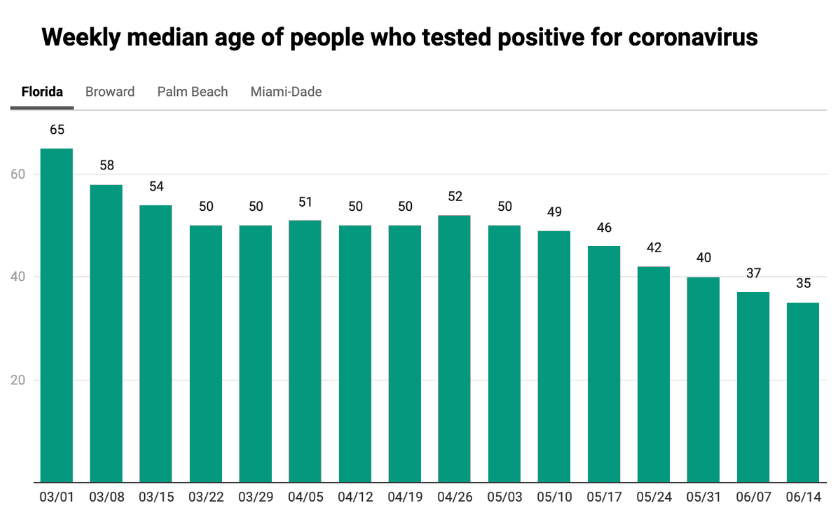
The starkest example, Florida, has actually slowed testing almost 10 percent, week over week, while seeing a 65 percent jump in the cases in the same time span. Florida’s rising cases, we can conclude, have nothing to do with expanded testing. South Carolina and Kentucky have followed the same pattern as Florida, with testing increases slowing while cases rise.
Given the high percent-positive rates and the degree to which case counts have outpaced tests in Arizona, Florida, and Texas, we interpret the case counts as indicators of sharply worsening outbreaks. In California and Georgia, where percent-positive rates remain relatively steady, the numbers are more difficult to interpret, but we’ll be watching them closely over the coming weeks.
What About Median Age and Demographics?
I came across a new article yesterday evening that sheds more light on the matter.
Death Trends Hard to Understand
Please consider Why Changing COVID-19 Demographics in the US Make Death Trends Harder to Understand.
On June 18, new daily COVID-19 cases in the US exceeded 27,000 for the first time since May 8, and stayed over 27,000 for the next four days. This was the first five-day run of new cases above that number since April 22-26. The 32,325 new cases reported on June 20 were the most since May 1, when just over 33,000 cases were reported. After plateauing in May, the trend is heading in the wrong direction.
Deaths, on the other hand, continue to decline: from June 18-22, fewer than 700 people in the US died each day, a first for a five-day period since March. The disconnect between case and death trends is striking; in Brazil and India, the two other large countries reporting a rapid increase in infections, in recent weeks as well.
Some anecdotal and statistical evidence suggests that the average age of people with COVID-19 is declining, which complicates expectations that deaths will increase in step with new cases.
In a Twitter thread, University of Florida biostatistics professor Dr. Natalie Dean offers three possible explanations for why the median age of cases might be falling, and what data signals we should look for.
Natalie Dean – Three Explanations of Rising Cases
- If it’s simply a matter of More Testing, hospitalizations should not increase, and test positivity should decline or hold steady. In the South and West, positivity rates appear to be rising, but regional numbers can mask very different state trends. In Texas, Florida, and Arizona, test positivity and cases are both rising; in California, by contrast, new cases are way up but the positivity rate has remained at five percent in June, and in Georgia the positivity rate is up just two percentage points while testing is up.
- If “elderly people are More Cautious,” then cases, test positivity, and hospitalizations should decline. In the Northeast, tests are way up, positivity is way down, and new cases are flat. In New Jersey, new daily cases are down to 10% of April peaks, and hospitalizations have dropped precipitously. New daily cases in Connecticut have been in the double digits for the past couple weeks, and hospitalizations are down to 124 as of June 23 from over a thousand in mid-May.
- If younger people are —or if they’re more exposed as young service workers return to their jobs—cases, test positivity, and hospitalizations should rise. This is happening in Texas and Arizona. Cases and test positivity are up in Florida; statewide hospital data was only available for a few days in May before the state removed it from public view, but in Miami-Dade County, hospitalizations increased from 601 to 776 from June 9 to June 22.
Dean ultimately concludes that it’s slightly too early to tell, but the real answer is likely a combination of all three, and that better age-stratified data is needed. High-quality samples exist for the country as a whole, but as we’ve seen, trends vary greatly from state to state and even city to city. The United States is a big country that needs a lot of detailed data.
Here is Dean’s 10-Point Twitter Thread
Three Points I Made
- Regional numbers mask trends.
- Hospital cases are rising and ICU beds are at capacity in Houston.
- We do not have Florida data because governor DeSantis blocked it, I believe on purpose, but feel free to make your own conclusions.
Convention Moved
In regards to point 3, please recall that on June 2, Trump says he is ‘forced’ to move Republican National Convention out of North Carolina.
- President Donald Trump announced late Tuesday that the GOP is now “forced” to look for another state to host the Republican National Convention due to social distancing guidelines that would limit event capacity.
- While Trump did not specify in his tweet to where the convention will be moved, multiple governors and GOP officials from places such as Texas and Georgia immediately offered up their states as potential hosts when the saga over the location of the convention first broke out.
On June 11, Trump announced the Convention Would Move to Jacksonville.
How Convenient
Now isn’t that move special?
Florida just happens to be the key swing state in the election, and Governor DeSantis in a totally unrelated move suppressed Covid totals.
And I am the Tooth Fairy.
Death Rate Will Rise
The reasonable conclusion is the death rate will rise, the key point I made.
In retrospect, I asked the wrong question: When Will the Exploding Number of Cases Lead to More Deaths?
“How fast?” is a better question.
I do not know, nor does anyone else.
One thing we do know (should know) is that it is foolish to conclude this is behind us, a position I am bombarded with daily from those who repeatedly deny there is a problem at all.
Mish




























The recent wave of protests has presumably also contributed to the surge in infections.
So average age of confirmed cases are down, that means deaths will be down as well. This is just simple Bayesian statistics (conditional probability).
There is no other analysis necessary, to come to any other conclusion is simple cognitive dissonance.
Facts: 43% of US deaths were people in nursing homes. That is 11% of the cases = 43% of deaths.
There is really no other possible conclusion?
Also if ICU is filled in only one city in the entire USA, that is statistically irrelevant. You’d need full ICU’s in multiple locations.
Also they are treating it better now. No intubation (equals almost certain death for C19 patients) and other treatments have improved chances of survival.
CDC data showing this has flu level death rate.
It is a simple illusion at this point, mathematically.
Politically it is a different story as we appeared to have self-inflicted the great depression for nothing.
There are too many confounding variables to get a straight message from this data:
–The mortality rate is affected by improving therapeutic approaches.
–The mortality rate is affected by the demographics of those being infected.
–The testing gateway protocol is getting laxer, so more of the positives will belong to the group that does not become severely ill.
–Nation or statewide aggregation only serves to distort the picture. Epidemics affect disparate regions.
All in all, this means earlier and later data are not easily comparable. Any evaluation of the measures taken can only take place when the epidemic has run its course and the outcomes (not only on covid mortality) begin to crystallize.
Yesterday you said you were looking for a chart of hospitalizations vs deaths over time but cannot find one.
Twitter user Covid19crusher posted these charts 6/26:
He also posted this BBC report that says coronavirus death rate falling in hospitals:
Oh Jazus, there goes my hospital’s 39K bucks. Better call in the ‘electives’.
Mish, As noted there are a lot of moving pieces that will impact the death rate going forward, the biggest I believe is effective medical treatments…recent CREDIBLE medical studies have shown dramatic improvement in outcomes with the following treatments:
HCQ + (Immediately after infection…very effective but only if taken early)
Tocilizumab
Anakinra
Vitamin D (Get it directly from midday sun as well)
Vitamin C
Zinc
Elderberry Syrup
The average age is dropping for a number of reasons. Young healthy people realize they are not at risk and are willing to reengage socially. Infected elderly are no longer being readmitted to nursing homes unequipped to separate populations(40% of US deaths may have come from nursing homes). Those at high risk are now being better isolated. People are now wearing masks, washing hands and doing a better job of social distancing, so the viral loads of those infected may be less deadly.
Other wildcards. Has the virus already mutated? (The Italian version looks worse than that coming out of China). And will it mutate again?
HCQ – Nope, just the same quack in France that pushed it two months ago. And yeah no actual clinical studies.
This study just came out this week:
It is different from the US studies in that the HCQ was given early, as soon as the patient was diagnosed, and before they needed hospitalization. Another difference is that they monitored zinc levels.
When given early, HCQ decreased deaths, transfers to ICU, and the number of days of viral shedding. Average days hospitalized was reduced from 9.2 days to 7.3 days. Patients ending up in the ICU were reduced from 6.8% to .8%, and the death rate was reduced from 3.1% to 0.5%. In total, “poor clinical outcomes”, as defined by death, transfer to ICU, or hospitalization for over 10 days, was reduced from 17.6% to 3.9%.
The study is a retrospective, and not a double blind study. It also has a flaw that the patients on HCQ were somewhat younger and had less co-morbidities. The improvement in results was so dramatic, and so extreme, that the improvement can not be explained by the difference in the ages or co-morbidities, however.
The biggest problem with HCQ is that it is off patent, and is an inexpensive generic. In most countries that is a good thing, but not in the US. Don’t expect to see it used in the US, as there is no money in it.
Another think I have seen suggested as a possible preventative is Quercitin, which reduces the amount of furin. It also is a zinc ionophore, giving it two separate properties that might help protect against Covid19. As fringe benefits, it reduces allergy symptom severity and has been suspected of anti-cancer activity, as well as being useful if you have diabetes. The biggest problem with quercitin is that it is very poorly absorbed, and is not soluble in water.
The thing that really bothers me in this whole debate is the overall lack of knowledge about this virus and what is really at stake. People mistakenly are under the impression that you either die, or you survive and fully recover. That is not really the case. This virus leaves many survivors with lasting and sometimes lifelong damage to their health. The after effects of this virus are very serious and something almost no one understands. We really need to educate people about the long term health dangers of this virus and why you really do not want to risk contagion. Chances are good you will survive, but you may never be the same..
From NY Times today “It is impossible to calculate the human toll of that two-month delay, but models suggest that earlier action might have saved tens of thousands of lives. Though estimates vary, models using data from Hong Kong, Singapore and China suggest that 30 to 60 percent of spreading occurs when people have no symptoms.”
I ask – if SO much of Covid infection occurs in people with no symptoms isn’t the only way to slow the transmission to test as many as possible to cull out all the transmission from asymptomatic transmission? No? Prey tell, how do you then?
If I was in Florida I would be apoplectic at Governor DeSantis for hiding the hospitalization data. It is amoral in a time of societal crisis.
I consider this a legit and important question with all the new infections to ask:
What does it mean to test positive for covid? We know the potential illness/damage to ones body it can do but what about disclosure? Do you tell your friends/neighbors/co-workers/ employer? And how will they treat you? Hospitals/Drs ask patients if you have any covid symptoms/exposure. What about employers/insurance application questions? If you are covid positive are you the new pariah (e.g. HIV/HepC persons)?
Quote: Spouse’s partner whose family most likely had this, he won’t test because he fears it will be used against him, both for pre existing condition and work requirements.
A long range question–if a limited-time immunity is conferred by getting CV, will you be better able to handle getting it a second time, or will the damage done be additive each time you get it?
My guess is both. Your body will handle it better, but any damage will add to the damage already done. However, there his a third, and worse alternative, and that is that, having seen it once before, your body will immediately jump into the over-reaction phase, and you go directly to the cytokine storm. Let’s hope that isn’t what happens.
Gilteritnib, Ralimetinib, Remdesivir…
The only problem with these sorts of drugs is they are near the limits of human tolerability and come with all sorts of side effects. Cancer treatments are quite often a balance of suppressing/killing the cancer and killing you.
Chlorox.
Sorry those medicines arent as lethal as cancer treatments which kill all cells. Antivirals are our best hope.
You are correct that anti-retroviral drugs are the best hope identified so far, but they’re also aggressive chemotherapies. Their long-term use in HIV patients have led to lots of side-effects. Those side-effects are still preferable to developing AIDS and full immune system collapse, but they’re no fun themselves.
These drugs are for those on ventilators with only about a 30% chance of getting out of the ICU alive.
New treatments and prophylactics are always good news but at this point there seems to me to be 2 points about the recent spike in light of the age profile.
First, this is a dangerous disease that is potentially life altering if contracted and death is just the top-end crisis. Concentrating on death rate seems flawed to me because it is a serious disease for any age group that, again, can have life altering consequences if contracted.
Then, if the age group that is spiking is the thirty-somethings, the mass of infection will slosh around and eventually find and hit the most vulnerable and show up in the death rate but later down road. (As I now see Clover NL mentions above.)
You’re right, Mish, that the death lag involves many factors. In addition to the factors you mention,
Looks like Kinase inhibitors will work the best to beat back Covid-19 and work better than even Remdesivir (which was only 30% effective in the worst cases). So far this is the best approach to understanding and beating back Covid-19. A vaccine won’t do anything and it may make things worse because it would give Covid-19 to healthy people. Covid-19 replicates and attacks very quickly and antibodies disappear within months.
By focusing on the fundamental behavior of the virus — how it hijacks key human proteins and uses them to benefit itself and harm us — the team was able to identify a family of existing drugs called kinase inhibitors that appear to offer the most effective treatment yet for COVID-19.
“We’ve tested a number of these kinase inhibitors and some are better than remdesivir,” said Nevan Krogan, one of more than 70 authors of the new paper, and director of the Quantitative Biosciences Institute at the University of California, San Francisco.
While remdesivir has yet to be approved for use against COVID-19, U.S. regulators are allowing “emergency use” of the drug in hospitalized patients.
Krogan said tests of kinase inhibitors showed some, including Gilteritnib and Ralimetinib, required lower concentrations than remdesivir in order to kill off 50% of the virus.
The new study, which involved experiments using cells from humans and others from African green monkeys, shows that the virus known as SARS-CoV-2 is especially adept at disrupting vital communications. These communications take place both within cells and from one cell to another.
A treatment doesn’t have to be very good to be better than Remdesivir, which showed no significant improvement in death rate, but only an improvement in speed of recovery. Partly that is because, since it can only be administered by IV, it can’t be administered until late in the infection.
The remdesivir study of the worst cases showed cutting death rate by 30%. That’s the real thing. Most people won’t need these medicines.
This is the only study of Remdesiver that I have seen that was positive:
Death for people taking Remdesiver were slightly lower than the deaths for the control group, but were not statistically significant because the reduction was small relative to the sample size. Was there a later study that I missed that showed a reduction in deaths? If so, could you link it?
Kinase inhibitors are used to treat late-stage HIV infections. SARS-CoV-2 also masks its presence in cells from the immune system using a similar method to HIV.
“We do not have Florida data because governor DeSantis blocked it”
This, and ambulance chaser ran kangaroo courts having an even theoretically possible say in who publishes what and “makes money off it”, is what pliantly stupid, well indoctrinated Newspeakers in totalitarian dystopias, are told to wrap themselves in a flag and call “But we have freedom of speech….”
“The median age in positive test cases is declining. But what does it mean?”
…
Long term health care costs?
Frankly, initial studies showing organ damage in even asymptomatic people worrisome. This virus is way to novel to know long term effects. Maybe, things will prove not that bad. But we don’t just know yet.
The trajectory of the disease in the US according to a certain demographic…
First–its a hoax
Then–its exaggerated
Then–NYC is different than everywhere else
Then–its only old people
Then–masks are for sissies and commies
Then–it’ll just go away
Then–sun and heat will make it go
Then–see it was nothing, lets party
Then–too much testing
Now–its only young people-there wont be more deaths
Wrong so many time before, but still noisily hammering away at it like the world’s worst carpenter building the world’s worst outhouse.
Reading Market Ticker?
Don’t ask me why, but I get a guilty pleasure reading Krazy Karl.
He is so wrong on so many things, yet he still has his sycophants.
For a long time he was pounding the table telling folks to go long Blackberry (RIM) and short Apple.
Hhmm, I haven’t heard him bring that trade up in years …
Denninger would be a hilarious read if the impact of his latest rhetoric on COVID wasn’t so dire.
An idiot following his advice to go long on BBRY and short on AAPL would simply have a margin call and an empty brokerage account.
An idiot following his advice on COVID-19 could end up infecting vulnerable people and killing them.
You missed “The only way to stop it is herd immunity, and we will all catch it sooner or later, so let’s spread it faster”. [But, other countries have stopped it, so this is another one that is wrong.]
And eventually, it will be “why can’t I get an ICU bed for myself/my spouse/my child? The LIBERALS in the coastal areas are responsible for the shortage!”
Death rates dropping because, hopefully, treatment regimes are improving. But as the Captain says old folk are being more cautious. And early testing rates were abysmal, so mostly only the sick were being tested. With wider testing a more accurate demographic of the infected becomes apparent.
But that +ve rates of 5% are still common indicates that the virus is near enough to endemic in the many parts of the US. So getting close to having to give up on containment and address living with COVID-19.
There has been some discussion on differences in virulence in the strains that appeared in Wuhan and then to West Coast USA those that spread to Europe and then to East Coast USA. That the latter was more fatal, but that over time the less deadly strains will spread cos killing your host quickly is bad. Which may also lead to lower death rates.
But.. this virus seems to have some nastier tricks than common coronavirii so as a larger population is infected the greater the chance of a outbreaks of more deadly strains.
WTF. Treatment regimes improving? The implication of that statement is that we have this under control which is not true at all.
Treatment regimens are absolutely improving. That doesn’t mean they can’t continue to improve, and obviously we all hope they continue to improve. Initially, for example, people placed on ventilators had a 12% chance of surviving. Now it is 71%. I’d call that a significant improvement.
” So getting close to having to give up on containment and address living with COVID-19″
Note: ” In the Northeast, tests are way up, positivity is way down, and new cases are flat. In New Jersey, new daily cases are down to 10% of April peaks, and hospitalizations have dropped precipitously. New daily cases in Connecticut have been in the double digits for the past couple weeks, and hospitalizations are down to 124 as of June 23 from over a thousand in mid-May.”
Seems like that is a path to getting it under control. “Was it over when the Germans bombed Pearl Harbor?”
As a resident in a small town in South Carolina, what I see every day is exactly what I’d expect: the closer one is to end-of-life, the more careful.
Alpha Group: goes to restaurants etc regardless of crowds, no masks, no distancing. High percentage of young adults and families.
Omega Group: typically older, they continue to social distance, make minimum trips and wear masks to the store.