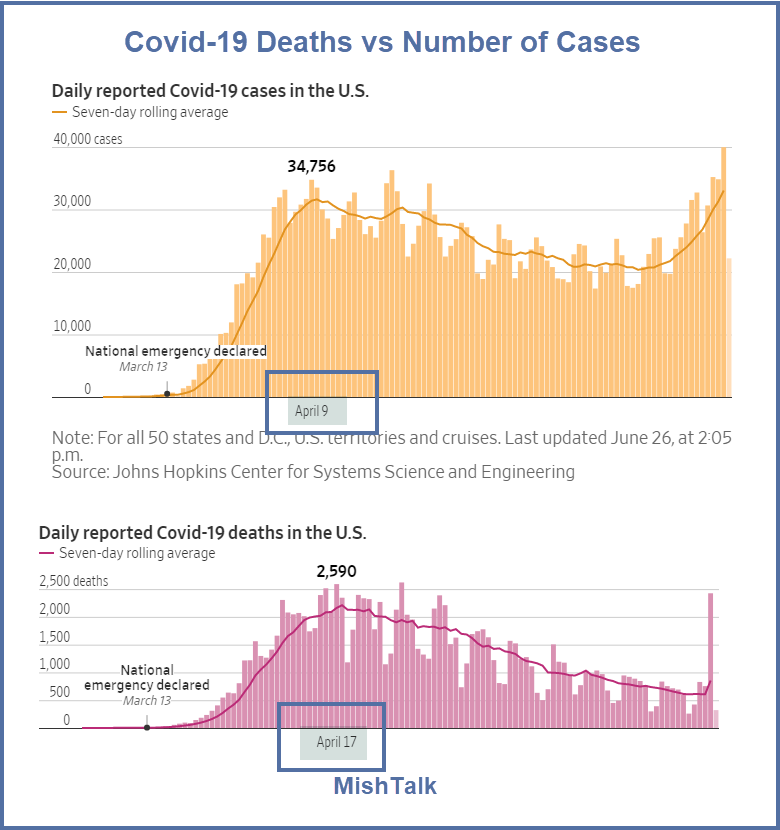
The 7-day average in cases peaked on April 9 at 34,756. The number of deaths per day peaked at 2,590 eight days later.
To suggest a lag of about a week is wrong.
Key Reasons the Lag isn’t a Week
- States did not peak at the same time. Averaging the states together smoothed out the curve.
- States had different reporting methods. Some states lumped probable deaths in with known deaths.
- Some states purposely downplayed deaths.
If is highly likely Florida artificially and purposely undercounted Covid deaths.
The Tampa Bay Times reports Florida medical examiners were releasing coronavirus death data. The state made them stop.
When the medical examiners’ list was available, it showed more deaths than the state’s count.
The Palm Beach Post editorial says Gov. DeSantis still hiding crucial data on COVID-19 deaths from the public.
The number of cases are now too many to hide.
Fools’ Analysis

Typical Reaction to Bad Analysis
Federal Reopening Criteria
Distorted “Real World” Methodology Explained

The proper way to compare death rates is to pay heed to state-by-state variations and lag rates.
Lag Time in Florida

It took over a month before deaths caught up to the original surge in Florida Covid-cases.
Lag Time in New York

New York had the smallest lag time. It was less than a week.
Lag Time in Arizona

Arizona had so few cases that it is a stretch to point out a lag time. But an explosion of cases started at the end of May and on June 24 there was a meaningful new record high in the 7-day average number of deaths.
Both of these lags are about three weeks.
Lag Time in California

California is similar to Arizona. It has weak relationships as well, if not more so. But to dismiss the rising number of cases as meaningless is folly.
Lag Time in New Jersey

New Jersey is either a double top of two separate cases or a longer lag of about three weeks.
Texas Lag Time

The initial lag time in Texas was a month.
National Lag vs State Lags
- Florida has a lag time of 5 weeks
- Texas a lag time of 4-5 weeks
- New Jersey a rolling top of 3 weeks.
- It is hard to say what the lag time is in California and Arizona.
- New York has a small lag of about a week.
- Average all of this together you get a national lag time of 8 days.
Comment From Nate Silver
Rise Not Due to More Testing
Stats That Allegedly Do Not Matter

Most of those are record highs. But hey, it cannot possibly matter.
Disbeliever Tactics
The disbelievers generally do not factor in that fact that lags can be a month or more.
Nor do they accept the proven fact that social distancing works.
We can debate the price tag but it is proven foolishness to suggest that social distancing does work.
Governors in Florida, Texas, and Arizona casually disregarded and downplayed social distancing.
So did mayors in various cities in California. And so did president Trump.
This Will Soon Go Away
Please play that video for an amusing flashback.
Look what happened.
Panic in Texas and Other Responses
- Texas Shuts Bars at Noon as Covid Cases Surge
- Houston Exceeds ICU Capacity
- EU Lifts Its Travel Ban But Not For the US
- Florida Closes Bars in Response to Covid Spike and NBA Season Threatened
- Trump is Behind in Every Recent Battleground Poll and his Covid handling is one of the reasons.
Fake “Real World” vs Real “Real World”
In the fake “real world” we can ignore the exploding number of cases, just as Trump did in late February and early March.
In the real “real world” things are just a bit more complicated.
Mish




























Deaths to October 9
The “We can debate” sentence is missing a neagation.
Mish, saw this at CNBC today and wow is it damning for red states that ignored warnings:
Notice that every state in the sharp increase category is a red state and the the blue states that did impose sharp restrictions are all now contributing only a small fraction of the uptick.
A four week lag seems right. Even if this wave has more young people, they will infect their parents and grandparents soon enough. Family spread is something that all successful countries dealt with and the US is doing nothing so family spread will blow out the death rate once again.
Studies will be done on long term health problems from covid for survivors.
It is obvious that masks and social distancing help.
There is little-to-no price to using masks in crowded spaces.
One can make the argument that the price of social distancing is too high as younger people as up to 40s are hardly impacted.
However, there are social activities which are less critical. I’d argue that we can live w/o movie theaters and bars. Schooling of pre-K and elementary is quite critical. Middle and high school could manage online – maybe with one day per week attending the actual school facility in person. This might not suffice for kids with poor conditions at home, though. Etc.
The only death the Federal government seems to be worried about is the financial system.
The view from Ventura County:
” it is proven foolishness to suggest that social distancing does [NOT] work. “
I echo the other commenter who critiqued your use of the term ‘disbeliever.’ As you yourself know better than most – because it is your skillset – sorting through the data available is difficult. The standards for such data are all over the map. You say CV19 is under-reported, many others say it is over-reported. These things can go round and round forever.
The root problem that the term ‘disbelief’ correctly indicates is that it all DOES come down to belief. Again, given that precise definitions for what constitutes a covid death are lacking and so counting criteria vary widely. Efficacy of tests vary widely as well (there is occasional reference in the literature about how the false positive rate is far higher than generally admitted, and now also occasional reports about how there may be far more widespread immunity already in the population from previous covid episodes – which may explain in part Asia’s greater success numbers-wise along with being prepared after the last SARS whereas we were not.
In theory, we should have excellent data so we wouldn’t have to throw around such terms as ‘disbeliever’ and ‘believer’ but as it is, that’s what we are left with. One of the greatest failures of Team Fauxi, imo.
Baron, Dr. Quack here, I’m setting up a new website under my moniker: ‘Cure(s) for covid RELATED illness’. I’ll will offer any number of nostrums from my prior efforts (backaches, joint recovery, you-name-it); any help here??? Hey, if the US gov’t can offer hospitals 39K for every RELATED covid illness, can’t I join the effort, hmmm?
Have no idea what your post means.
Quick search. For a while the figures were batted around in the media and as with all figures nowadays, some disagree. It’s $39,000 for those on ventilators, only $13,000 for CV 19. Still, it’s money. Assuming that extra kick has no effect on statistics is absurdly naive.
Keep a watch for this statement: ‘Covid Related’.
There are lies, damned lies and statistics!!
Without the latter, there would have been little awareness of this entire thing which – outside NY & NJ, was basically less than a bad flu season. In NY, they packed people in old peoples’ centers – for which there should be criminal indictments – and the entire shutdown approach will probably cause more and earlier deaths for many years to come than the virus, plus the political fallout from so draconian, protracted and cowardly a response has probably ruined any chance for a good future for our progeny.
Yup, them thar statistics are dangerous things, Alfie!!!
In the particular case of Covid19, nobody seems to be paying attention.
If you believe that an infected individual becomes infectious after 2 days (3 days prior to showing symptoms) and if you believe the infection rate is 3 then the arithmetic looks something like this:
Day 1 – 1 infected person (we make abstraction here as to how this person got infected)
Day 3 – 4 infected persons (the original person infected + 3 new infected individuals)
Day 5 – 16 infected individuals (4 earlier infected individuals x 3 + 4 original individuals)
Day 7 – 64 (16 x 3 + 16)
Day 9 – 256
Day 11 – 1024
Given the assumptions, this progression gives you more than 80 million infected individuals in 31 days.
This is basic math.
If there is any debate to be had, it is whether or not this progression is correct. Anything else only leads to bickering and recriminations.
Is the arithmetical progression of the infection correct or not? Nothing else matters.
If the math is correct, then:
As we are finding out that this virus has been circulating since fall 2019 or even summer 2019 the math tells you a number of things.
The first thing you can infer is that, given the progression as outlined above, the virus is already well spread throughout the global population.
That being the case, the first realisation is that blanket confinements of the population 3 months or even 1 month after realising a new bug is on the scene is, arithmetically speaking, not very useful.
The second thing you can infer is that, given the progression as outlined above, the population must already have some degree of immunity. We can infer so by the fact that if the entire population was susceptible to this virus, we would have had significantly more hospitalisations and deaths; we are talking orders of magnitude here. This would have been particularly so aboard all the ships where Covid19 was detected. Yet, of all the ships identified as being infected with Covid19, the Diamond Princess is the one that reported the highest infection rate with just under 800 infections out of a population of 3500. But the more interesting case is highlighted by The Zaandam. The Zaandam was stranded at sea for a total of 23 days. During this time, first flu-like symptoms manifested on day 14. It is only on day 15 that the captain issued confinement orders. By the end of the whole sorry saga, 23 days had elapsed. 23 days during which the population of The Zaandam had been completely isolated, at sea, far from anyone anywhere in the world and where, during 14 days straight, passengers and crew mingled happily without a care in the world. Yet, The Zaandam presents us with infections of fewer than 100 out of a population of 2000 passengers and crew…. and 4 fatalities of which only 2 tested positive for Covid19.
The third thing we can infer from the above is that regardless of what you think of masks, given the arithmetical progression as above, wearing masks will change little.
Finally, although the spread of the virus may, to a degree, have been slowed by confining the population, three things should be glaringly obvious:
1 Confinement does not eradicate the virus. Confinement can merely slow down the contagion. So, albeit at a slower pace (i.e. Ro of 1.4), contagion progresses. Due to the compounding nature of contagion however, confining the population merely buys you a handful of days time as compared to not mandating blanker confinements. But progress the virus will nonetheless.
2 Wearing masks does not eradicate the virus. So, albeit at a slower pace, contagion progresses. Due to the compounding nature of contagion however, wearing masks merely buys you a handful of days time. But progress the virus will nonetheless.
3 Even assuming we could put out a vaccine today, it will be many months, if not years, till the entire global population can be vaccinated to a reasonable degree. In the meantime, the arithmetical progression as outlined above, continues.
So, unless you can dispute the arithmetical progression as outlined above, confinements and mask wearing may make you feel good. The reality however is that it makes little difference.
So the entire debate should hinge on whether we do or do not have the arithmetical progression right.
Everything else only results in unnecessary bickering and recriminations.
So, can we or can we not agree on the arithmetical progression of the infection?
If we look at countries and states that have required masks, we have real world data, and that is better than entirely speculative math. In the real world, every country, and every state, that has required masks, has shown declining infections and deaths. Wearing masks does not totally stop the spread, but it reduces the R0 to below 1.0, and the virus dies out on it’s own.
The infection rate on ships is not speculative. Three months after the fact, mortality can be speculative. Infections however, are not.
Reducing the Ro to below 1 does not eradicate the virus. The virus does not just die out.
The point of the exercise is to demonstrate that due to the progression of the contagion, or lack thereof, there is a degree of innate immunity in the population. The why and wherefore of it all is yet to be ascertained. What is clear however is that what happened on the ships, all the ships, including the war ships, demonstrates that the infection rate of Covid19 is limited.
In this regard, the work of Isaac Ben Israel and Prof. Michale Levitt (Nobel) is interesting. They both found that for whatever reason, this virus does not progress ad infinitum.
This is also evidenced by the fact that it is highly improbable that we have detected this new virus within days of it appearing on the scene.
It takes time to identify a new virus. If a new virus produces symptoms that are similar to other more common viruses, it takes even longer. It takes several cases and a lot of head scratching to realise that despite the fact that the symptoms are similar, the outcome is different.
By the time you think you have a new virus on your hands, it takes time for the medical profession to come around to that same realisation.
In the meantime, the virus is making inroads into the population.
Whether the Ro is 1.1, 3, 4 or 5 matters little. These are compounding progressions that very quickly go parabolic.
But the virus does not just die out. What can happen is that the population learns to live with it due to a vaccine or due to immunity.
The virus cannot just die out.
Since we don’t even know the method where the virus was being transmitted on the ships, it is a great leap of faith to make any projections about them. I think it is likely that, had they not gotten the people off of the ship, eventually everyone would have been infected. How long would that have taken? It depends on what the method of transmission was, and whether some people, by virtue of their location in the ships, or by virtue of their personal precautions, were more able to protect themselves than others.
Why were the infections on the Zaandam so much less than on the Diamond Princess? It would be illogical to conclude that everyone on the Zaandam was immune. The most logical conclusion is that there was something different about the design of the ship, or about the quarantine procedures, that led to that result. Again, we don’t know he transmission method, so everything becomes speculation. Were aerosolized virus particles passed in the air handler, or though the plumbing? Were virus particles passed on dishes? Were people exposed in stairwells and elevators? Any of these things could have been very different on the Zaandam than on the Diamond Princess by virtue of the design of the ship or company procedures.
There are certainly conclusions you can draw from the Diamond Princess. You can draw conclusions about the percentage of asymptomatic cases, and about the death rate. What you can’t draw is conclusions is whether the people who were not infected were immune, or simply not infected yet. You can, however, draw a reverse inference. Since 25% of the people were infected, and more were being infected every day, we can know that over 25% of people are susceptible, meaning that we are far, far from herd immunity in the real world.
You say “Whether the Ro is 1.1, 3, 4 or 5 matters little.” It does matter a lot, though. The higher the native R0 is, the more steps must be taken if you want to get it below 1.0. If you get it down to .8, then first cycle you have 100 cases, then 80, then 64, then 51, then 41, 32, 26, 21, and so on, until you after 20 cycles, you have less than 1, meaning no more cases. Now, how do you get to less than 1.0? Some suggest ignoring it and letting it spread until you achieve herd immunity. Others want to continue a lockdown. Others want to require masks.
The most important lesson we have learned in this pandemic is that, while lockdown work, requiring masks works just as well, without having a negative effect on the economy. Once the pandemic is over, we can go back and look at the data, including the costs of loss of people to death, the costs of treating the sick people, the costs of the disabilities induced by Covid, and the costs of the economic disruptions. Will the costs be lower in country like New Zealand, that had a hard lockdown until it was completely eliminated? Will it be lower in a country like Sweden that didn’t lock down at all, and tried to achieve herd immunity? Will it be lower in a country like Czechia that immediately adopted a rule requiring masks? My guess is that when it is all said and done, the pandemic will have had the least disruption in the countries that required masks, and the most disruptions in countries like Brazil and Sweden that just let it run, and in the middle will be countries like New Zealand that conquered the virus via lockdown. But, we’ll have to wait until it’s over before we know the outcome.
By the way, the other, very significant thing that you miss in your dismissal of masks, is that when sick people wear masks, while some virus particles do escape, they escape in smaller numbers. Thus, someone who is exposed is not only less likely to become infected, if he does get infected, he gets a smaller initial dose, or inoculum. A smaller initial does is more apt to lead to a mild case. Why? It takes more cycles of replication inside your body to get to the millions of particles it needs to cause symptoms. More cycles means more time for your body to react, and to mount a defense. Since one of the things that SARS-COV2 does is to weaken your immune system, allowing your immune system a head start gives you a much better chance for a mild case. Consider that before there was a vaccine for smallpox, for hundreds of years it was common practice to deliberately infect people with a very tiny dose of live virus, hoping to stimulate a mild case that would lead to lifetime protection.
In the end, you have the indisputable fact, and that is that masks save lives.
“It wasn’t just by a few per cent, it was up to a hundred times less mortality. The countries that introduced masks from the very beginning of their outbreak have had hardly any deaths.”
“The virus cannot just die out.”
Correct. But it’s virulence – the effect on us – does, nearly every time.
That is what matters, not whether or not it is still around.
In Italy, more people have the virus now but hardly anyone is sick any more. Same is happening in the States, though a recent surge from sick people coming over from peaking Mexico is spiked things up in a minor – albeit measurable – way. All over in a couple of weeks.
Mish, that last sentence should end “does not work” (delete my comment after correction):
The disbelievers generally do not factor in that fact that lags can be a month or more.
Nor do they accept the proven fact that social distancing works.
We can debate the price tag but it is proven foolishness to suggest that social distancing does work.
Mish, I would not worry till few “Hollywood Elites” crock of COVID-19 and,I read and confirm the report on TMZ, that when Meryll Creep,Robert D and few Pedophiles have final stages of COVID-19 in the Hollywood and come out and announce they are infected and are dying, that when I will start panicking, till then enjoy few shots of vodka.
My sincere apologies for a previous note wherein I disparaged tests. Please forgive me, I relent. Just today I heard that Dr. Fauci (I now use the Dr. in addition to the patronym or whatever he goes by) said he is about to institute a double test. The first will be a blanket test using a ‘proven’ methodology to, well, blanket the population (understandably the field grazed by the flocks), followed by the more trad swab test on those individuals ‘captured’ by the blanket effort. Oh! wonders! As my granddaughter says: two is more than one. Honey, two is better than one!
This is why we can’t have nice things….
Mish, you are fortunate to have so many epidemiologists among your readership. /sarc
I wish I was as certain about anything as some of your readers seem to be about everything.
Keep up the good work. Illegitimi non carborundum .
Statistics in the cornerstone of science and medicine. A lot can be understood from the data without The use of a medical degree.
The sad part about a lot of these comments is that it isn’t understood that effects are not instantaneous. It’s like turning asupertanker
The spike in cases is coming about a month after opening up.
And we all know that you don’t die the instant you get CV.
The spike in deaths will be at least two to three weeks from now.
In one month from now we will all know for sure.
I will be rooting for no spike in deaths. But given the evidence from other places it is quite possible.
What does it mean to test positive for covid? I know the potential illness/damage to ones body it can do but what about disclosure? Do you tell your friends/neighbors/co-workers/employers? And how will they treat you? If you are covid positive are you the new pariah?
WHATEVER the lag time, it is bound to bite both Pence & King Chaos in the ass, to claim NOW, that things are going well. https://www.cnn.com/2020/06/26/politics/fact-check-pence-briefing-coronavirus-june/index.html
The Russians and the Chinese are behind the latest increase in cases. I mean both Dems and Republicans can’t be wrong right?
Mish, your chart of daily death has a spurious data point that doesn’t belong there. It shows a jump to about 2400 a couple days ago that never happpened. The daily deaths the last few days have been:
June 22, 369
June 23, 871
June 24, 819
June 25, 653
June 26, 663
Oddly, there was a community post that claimed death had jumped over 2400 on Wednesday, and for documentation, he linked an article from the Washington Post. The article he linked was dated 4/25. Indeed, the deaths on Wednesday, 4/22, did top 2400, hitting 2409, but that’s rather old news, and shouldn’t be shows on the chart for this this week. (If you doubt that the Washington Post article was from 4/25, look at the URL.)
Edit – In further discussions, it appears that New Jersey went back and looked at all deaths since the start of the pandemic, and classified another 1900 deaths as “probable Covid deaths”. The spike on your chart reflects those additional 1900 deaths. It’s important to remember that they aren’t current deaths, but rather, deaths from March-April that were retroactively classified as Covid.
Mish,
I said it a few weeks ago, and I’ll say it again: you’re slipping. I used to read you blog every day, now I rarely come by. You used to approach issues with a skeptical eye, but with anything virus related your approach lacks sound rational thought. Here’s but one example:
“The disbelievers do not factor in that fact that lags can be a month or more.
Nor do they accept the proven fact that social distancing works.”
Grouping everyone who disagrees with you as a “disbeliever” is not only childish, but it paints a broad brush against people who might agree with you on some points, but has competing arguments on others.
I think everyone should be wearing masks in indoor places, and crowded outdoor places. I believe that we’re not social distancing enough. That has zero to do with your first point, which happens to be wrong….
Your third point is based on faulty reasoning. Look at a simple chart of cases to deaths. It lags, but the two lines have diverged considerably, more so than can be explained away by your conspiracy theory that deaths in Republican states are being hidden, or any of the other flimsy garbage you posted. Younger people are making up a larger percentage of cases in this round, as compared to NYC.
Apologies offered for missing the word generally.
“The disbelievers generally do not factor in that fact that lags can be a month or more.”
And believe what you want about Florida “garbage”
But there is a lot more than that regarding whistleblowers that I did not even post.
Re. 1.
That is the Trumpiness thing you all seem to go on about.
“Disbelievers” don’t factor in lags, “disbelievers” don’t agree with precautions . So “disbelievers” are those that meet both criteria, but you only meet one, does that make you a “disbeliever”? So there you have a classic example of the friend of the enemy style presentation which polarises position. Now Mish (probably) did not mean it like that, but has either picked it up from his favourite president without meaning to, maybe a kind of Freudian adulation he is unaware of, or everyone is so triggered that the moment they feel like they are being boxed into the wrong side, or even a side, they get upset immediately. I don’t know, but it is certainly amusing, in a precarious sort of way, to witness 🙂
I agree with you absolutely, and thank you for posting. I also noticed that Mish has apparently developed a less than critical attitude over the past many months. It’s like there is another virus circulating that short circuits reason. Anyway, we are in the minority, and no amount of evidence will turn the tide. Best wishes. Brian
I’ve been reading this blog for over a decade, and have done so because he is an exceptionally critical thinker. On the virus issue I feel like I’m reading Don Lemon.
I want a chart of hospitalizations ve deaths over time but cannot find one
Last chart at
?
This is for Florida but data source link given underneath probably has for US.
There may be no immunity against Covid-19, new Wuhan study suggests
Thanks for posting data
You cannot predict change in death rate without knowing the age of the new cases. If they are under 75, there will be no uptick in deaths. If they are asymptomatic with a positive antibody test, no uptick in deaths.
Just simple conditional probability. But people don’t like math so more hysteria.
Said another way – you CANNOT predict future deaths with CONFIRMED CASE statistics if you don’t adjust for (1) age; (2) age; (3) age; (4) in nursing home; (5) # of comorbidities.
A case on a person under 75 with no comorbids is 0.1% chance of death.
care to ignore surging ICU beds too?
If only in one or two hospitals nationwide, yes, obviously. If across the country, no.
I think the increase confirmed cases is due to more widespread testing. It is also simple math. We’ve seen statistics that in some areas of the USA where they’ve done random testing 25-30% of the population has the antibodies.
Initially only the very sick (and the very wealthy) presenting with severe symptoms in nursing homes and hospitals were tested. At that point, confirmed cases were highly correlated to risk of death (these were the riskiest and symptomatic people).
On Facebook there has been a lot of publicity (ESPECIALLY IN FL) for “Come in for a free test!”. That is going to bring in the asymptomatic (which recent research give evidence that they don’t spread it) and the people who’ve had it and its passed (i.e. younger people).
So there will be a BIG uptick in “confirmed cases” but it won’t be followed by a big uptick in deaths because these cases are those not at risk.
This is politics at this point, not Bayesian statistics.
Not ignoring but those same factors still play a role in determining survival even in the ICU. The virus is there’s, no one is arguing but if the majority of cases are younger and healthier, then so is the death rate. This is an old person’s disease!
“Health officials in Texas are logging every single COVID-19-positive hospital patient in the state as a COVID-19 hospitalization, even if the patients themselves are admitted seeking treatment for something other than the coronavirus…”
“Queries to multiple Texas hospital officials this week went unanswered. But leaders of several major hospitals in Houston this week urged the public to remain calm, suggesting that the extent of the outbreak has been overstated…”
“The number of hospitalizations are “being misinterpreted,” said Houston Methodist CEO Marc Boom, “and, quite frankly, we’re concerned that there is a level of alarm in the community that is unwarranted right now.”
“The time is now for everybody to dramatically change their behaviors to get this virus under control so that our hospitals for the weeks to come are there and able to handle this, and we feel confident we can as long as people act now and help bring the curve down over the next couple, three weeks,” Boom said.
There are also significant influx of dual citizens from Mexico as they peak right now:
If you look at the map where the most surges are happening, they are mainly border areas (including Florida, albeit by plane).
(Yes, the link is from Conservative Review regarded as highly partisan, but it is the never-Trumper bastion – albeit Horowitz is not of that ilk.)
Personally, I trust very few numbers coming out. However, as the dust settles, we can simply compare the typical daily or weekly death rate for that time of year with the current one to get an idea of how many extra deaths than usual we are suffering. A high percentage of CV19 deaths happen to those with co-morbidities, which in layman’s terms is very close to ‘they were about to die anyway.’ I found a week-to-week comparison chart early on in March but have not been able to locate one like it since.
I also read scattered articles a couple of weeks back about how in several countries – notably Italy but others too – it appears the virulence quotient is on the decline, i.e. those that get it now have far lower viral counts; therefore one can expect morbidity to keep declining.
To presume that this is purely a medical event and not also a political one is absurdly naive. We should all be careful what we are wishing for here.
If anyone is interested in viewing the conference, you can find it here along with a local news report:
Iran case graph profile matched the US. Their lag was 3 to 4 weeks. Lots of invulnerable young people exposed, deaths followed 3 to 4 weeks later. See the attached graph….
The average age of the person in the newer cases is dramatically lower, so 10,000 new cases may mean 2-5 deaths instead of 30 or 40 as in April and May.
Exactly. In Florida, the average age is in the 30’s & 40’s for each county, and death rate has plummeted. Hospitals is at 4.8% for that demographic which is normal. Headlines say “17 new deaths” but the last death happened on 6/21. LTC’s are UP to 53%, but that’s the failure of whoever is in charge (still not close to the complete failure of MA & NY of 63% of deaths). But hey, the late 1960’s over a million died of a flu…/shrug
Since the 1900, these have been the worse flu epidemics in the US:
1.1918, Spanish flu, 675,000
2. 2020 Cornavirus, 127,000 and counting
3. 1957 Asian Flu, 116,000
4. 1968 Hong Kong Flu, 100,000
Be aware that at the end of the flu season, the CDC estimates the degree of undercounting, and then multiplies the recorded deaths by a factor to get the number it reports for the final number. For the flu, they normally multiply the recorded deaths by about 5. Covid numbers have been kept much more closely that for the normal flu, so I’m expected the factor to be less than 2, probably about 1.4.
That is part of what makes me question the new case numbers. I don’t go as far as Trump on that, but there is plenty of room to find changes in new cases, or to hide them, depending on testing. When it comes to comparing data between countries it is even more difficult, because of protocol, political presentation, number of tests available etc. I know it varies widely from country to country, even within same region.
For sure lack of precaution, ending lockdown and so on will see a rise in cases and fatalities, but there is so much room to fudge the numbers that to me it is all painted with a broad brush that only provides rough trends. In EU cases are picking up again, likely not too far off US eventually but who knows. Either way, if they want to micromanage the data and media they are going to have to micromanage the restart to avoid large outbreaks, I guess the two go together in terms of policy but they really cannot return to wide lockdowns again now, I don’t think people would tolerate it. Opening to travel beyond bare nescessity is probably not wise either if they want to control the outbreak. It isn’t just that visitors bring in new points of contagion (which is well documented) , it is more the wider mixing of society which will be taken as normal – after seeing that outsiders are allowed this . You cannot restrict travel indefinitely either, so who knows where this all leads.
Prediction:
Most issues around coronavirus – at least in the US but I suspect world wide – will rapidly resolve between Nov 3 – 10 2020.